GM CASES
50 year old female came with complaints of abdominal distension, shortness of breath, burning micturition, decreased appetite, nausea since 5 days and dry cough since yesterday.








 USG chest:
USG chest:
 2d echo:
2d echo:
 hemogram:
hemogram:

 Final diagnosis:
Final diagnosis:
History of present illness:
Patient was apparently asymptomatic 2 years back, then diagnosed with pancreatitis and AKI, for which she underwent 2 sessions of hemodialysis. At that time, she also tested positive for dengue.
2 months back, she tested positive for covid 19 and received medication at home. She was also diagnosed to be diabetic and hypertensive, but on irregular medication.
Now, she c/o abdominal distension, decreased appetite, nausea, burning micturition and sob on exertion (grade 2); for which she went to local hospital but her symptoms did not subside. So, she came here for better treatment.
No h/o palpitations, chest pain, fever, decreased urine output, pedal edema, orthopnea, PND, vomitings.
Past history:
Not a known case of asthma, TB, epilepsy, CAD, CVA, thyroid disorders.
No h/o surgeries and blood transfusions in the past.
Personal history:
She used to consume alcohol regularly. But she stopped 1 1/2 year back.
Family history:
No significant history
General examination:
Patient is conscious, coherent, co-operative
Moderately built and nourished
No signs of pallor, icterus, cyanosis, clubbing, koilonychia generalized lymphadenopathy, edema
Vitals at the time of admission:
Temp - 98.4 F
PR - 104 BPM, regular
RR - 16 cpm
BP - 90/60, after 1 bolus of IVF - 110/60
Spo2 - 99%
GRBS - 520 mg/dl
Systemic examination:
Per abdomen:
Abdomen is distended and soft
Diffuse tenderness present
No palpable masses
No free fluid
Hernial orifices - normal
Bowel sounds - heard
CVS:
S1, S2 Heard
No thrills, Murmurs
Respiratory system:
Trachea - Central
BAE+
NVBS heard
Decreased breath sound on right side
Basal crepitations +
CNS:
Speech - normal
No signs of meningeal irritation
Motor and sensory system: normal
Cranial nerves - intact
Reflexes - present
Plantar - flexor on both sides
Provisional Diagnosis:
Uncontrolled DM
UTI
Right lower lobe consolidation
With known case of type 2 DM and hypertension since 2 months
INVESTIGATIONS:
Urine for ketone bodies: negative
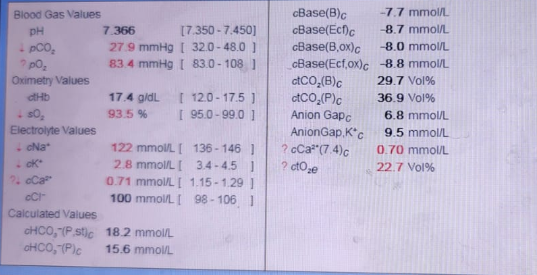
ABG:
Spot urine protein: creat ratio and urinary electrolytes:
RBS, LFT, RFT:
Chest x ray PA view:
X- ray Erect abdomen:
On 27-07-21:
RFT:
Serum amylase:
Seum lipase:
ESR:
HbA1C:
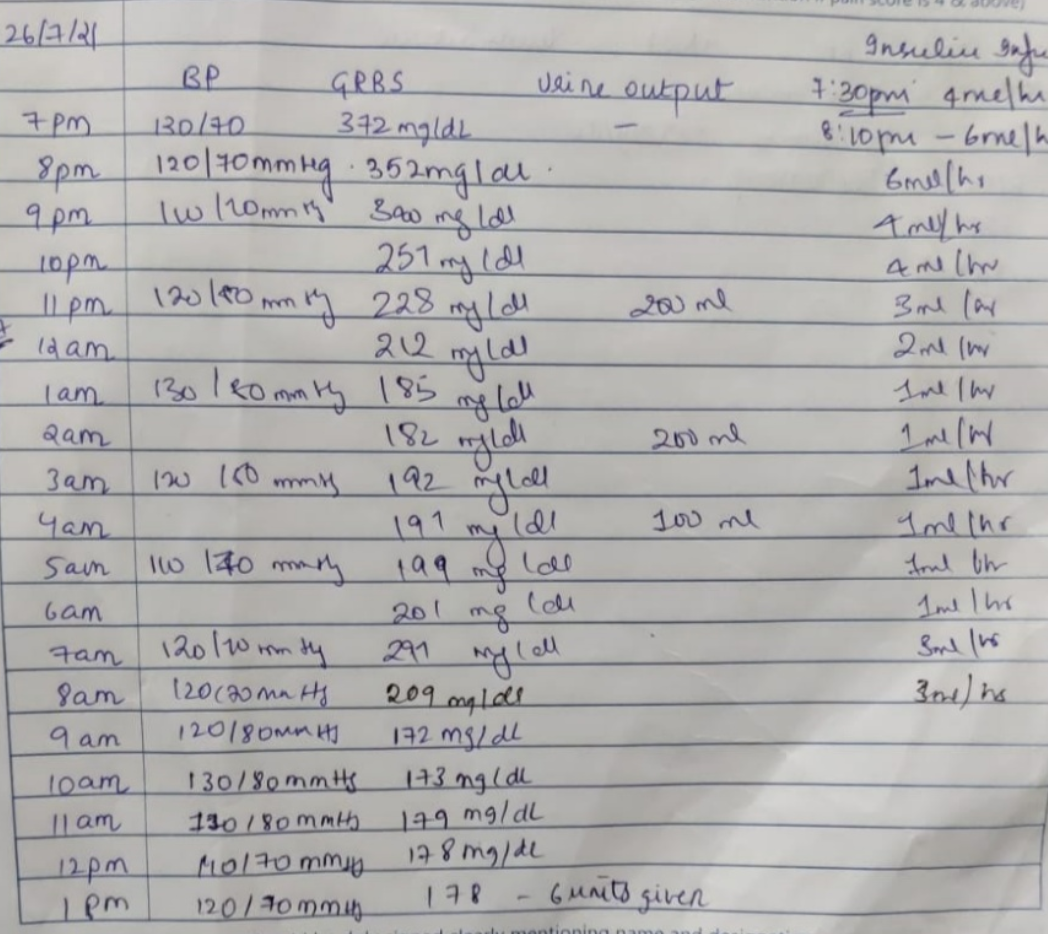
Blood sugar levels:
Uncontrolled DM
? Pneumonia ( post covid sequelae - fibrosis) (right lower lobe consolidation)
? UROSEPSIS
Treatment given:
Day 1:
1. IVF - NS @150ml/hr
2. NBM till further orders
3. Inj. 39 ml NS with 40IU HAI @6ml/hr
4. Hourly monitoring of GRBS levels
5. Strict I/O charting
Day 2:
1. Inj. PIPTAZ 4.5gm/IV/Stat f/b inj. PIPTAZ 2.5 gm/IV/TID
2. Inj. HAI SC/TID
3. Inj. PAN 40mg IV/OD
4. Inj. ZOFER 4mg IV/SOS
5. GRBS Charting 4th hourly
6. Tab. ULTRACET PO/QID
7. Syp. Ascoryl 10ml PO/TID


Comments
Post a Comment